|
|
The word describing the overall goal for HISP and the reason for HISP’s existence is empowerment. HISP want to empower the poor and marginalised through strengthening local health services in the developing world. Through training district health staff in gathering and analysing data, both for local use and reporting, HISP hopes to empower the district staff to give better service to their health district.
HISP is founded within the academic community and is therefor both research and action oriented. The research taking place within the HISP network is almost exclusively founded within the discipline of action research. The PhD and master students involved in HISP are adapting DHIS for the local context, train users, negotiate with health authorities and health workers and similar tasks needed to transfer the HISP methods and DHIS to a new region or new country. At the same time the researchers are collecting data for their thesis. There are health workers, ICT professionals and managers within the HISP network who is not tied to the academic community, but HISP have strong ties to this community.
Important to action research within the field of IS research is to involve all the people affected by the IS into the design, development and implementation of the system. The intension behind involving the affected parties into the process is to build a system more attuned to the users needs, and to instill a feeling of ownership towards the IS, thereby increasing the acceptance of the system. This is perceived more “democratic” than building a system in splendid isolation, and more likely to meet user’s needs. In the IS literature this is called participatory design.
An important factor for HISP in South Africa was the development of an EDS. Often the collection of data in the health systems in developing countries are data centric, which by consequence leads to lot of data being collected with little thought on the usefulness of the data. HISP promotes an action oriented approach to selecting which data to collect. Only data which can give information leading to action should be collected. This have given more focus to indicators and the data needed to calculate them. One example is immunisation coverage. To calculate this indicator you need to know how many children under one year have been fully immunized and how many children under one year living in the area. By challenging the data collected on usefulness an EDS is developed.
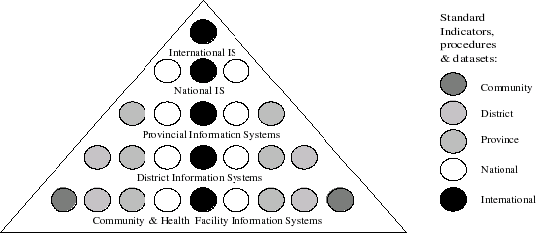
To empower local district staff and to lessen tension between what is perceived useful information by different actors in the health system, the model seen in figure 6.1 is promoted by HISP. The collection of routine data is often used to monitor and control the performance at lower levels in the hierarchy. This is an important part, but HISP want to promote local use of information. The combination of data used to report to higher levels and data perceived relevant only at the local level gives the hierarchy of standards for EDS, indicators and procedures in the figure. The size of the EDS grows less as it travels up the hierarchy. To support local use of information it is important that information is travelling both ways in the hierarchy. A region gathering data from the districts needs to report back data on the other districts to each respective district. In this way a district can compare itself to other districts, the regional total etc.
A multiplicity of simultaneous processes are taking place within HISP at the same time. There are nearly never any clear start or end to the processes taking place. The process of transfer takes different forms in the countries HISP are transfered to. The transfer of HISP to a new country is called a horizontal transfer. Within a country the process of vertical transfer are taking place. When HISP is transfered to a new region or districts, new and distinct processes are taking place. In Ethiopia the transfer of HISP to Addis Ababa was different from my experiences transferring HISP to the Tigray region. Three broad categories of processes taking place can be identified, however.
A paper authored by prominent actors within HISP (Braa et al. 2004) calls the approach used by HISP the networks of action approach. They conclude that this approach is better at addressing sustainability of intervention and is characterised by: